")
")
Olayiwola Akeem Bolaji1, Fariba Yazdanpanah1*, Anusha Kumari Battula1, Uchenna Declan Unamba1 and Bulent Zaim2
1Department of Internal Medicine, University of Maryland Capital Region Medical Center, 901 Harry S Truman Drive N, Largo, MD, 20774, USA
2Department of Cardiology, University of Maryland Capital Region Medical Center, 901 Harry S Truman Drive N, Largo, MD, 20774, USA
*Corresponding author: Fariba Yazdanpanah, Internal Medicine Department, University of Maryland Capital Region Medical Center, 901 Harry S Truman Dr N, Largo, MD, 20774, USA. E-mail: Far.p.yaz@gmail.com
Received: April 13, 2022; Accepted: April 21, 2022; Published: April 30, 2022
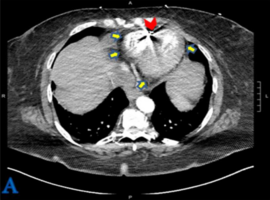
Citation: Bolaji OA, Yazdanpanah F, Battula AK, et al. Hole in Heart: An Unexpected Cause of Pleuritic Chest Pain. Clin Image Case Rep J. 2022; 4(4): 228.