")
")
Ling Oei1,2,3 and Sjaam Jainandunsing4*
1Department of Internal Medicine, Erasmus Medical Center, Rotterdam, The Netherlands
2Department of Internal Medicine, Leiden University Medical Center, Leiden, The Netherlands
3Department of Internal Medicine, Jan van Goyen Medical Center, Amsterdam, The Netherlands
4Department of Internal Medicine, Maasstad Hospital, Rotterdam, The Netherlands
*Corresponding author: Sjaam Jainandunsing, Department of Internal Medicine, Maasstad Hospital, Rotterdam, The Netherlands.
E-mail: jainandunsings@maasstadziekenhuis.nl
Received: October 30, 2022; Accepted: November 10, 2022; Published: November 19, 2022
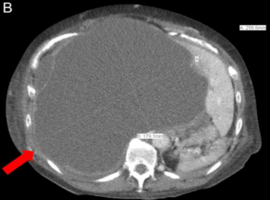
Citation: Oei L, Jainandunsing S. Hyponatremia Caused by Abdominal Large Vessel Obstruction. 2022; 4(11): 276.