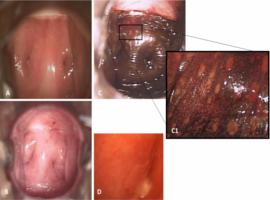
We report a 56-year-old healthy caucasian woman with a history of complete septate uterus, cervical duplication and non-obstructive longitudinal vaginal septum. In 2014, she had a cervical LSIL lesion in the left cervix (D) and was referred to our unit for surveillance and treatment. She was submitted to septotomy of the vaginal septum and excision of the LSIL lesion with CO2 LASER. The last cytology and HPV typing tests were negative. She is currently asymptomatic and under surveillance.
(A): Present colposcopic image, without preparation, where cervical duplication is identified. Application of acetic acid (B) and lugol solution (C). The exam revealed 2 cervix with type 3 transformation zone and an inflammatory punctation suggestive of diffuse and focal mixed colpitis (C1).
Inflammatory lesions of the cervix are not confined to the transformation zone and produce a nonspecific inflammatory response, which may include redness, vascular abnormalities, and varying degrees of epithelial desquamation [1]. In the same observation, signs suggestive of different infections may be present. In our case, focal punctation typically suggests a bacterial vaginosis, whereas diffuse colpitis with small punctation is more associated with candidiasis or even HPV sequelae.
Mixed colpitis and vaginitis represent a significant therapeutic challenge requiring initial dual antimicrobial therapy [2,3]. Our patient was treat with a nifuratel?nystatin combination and clindamycin.
")
")