")
")
Tomohito Shinoda, Tanahashi Toshiyuki* and Takuya Nakashima
Department of Surgery, Gifu Municipal Hospital, Kashimacho, Gifu, Japan
*Corresponding author: Toshiyuki Tanahashi, Department of Surgery, Gifu Municipal Hospital, Kashimacho, Gifu, Japan. E-mail: c2001049@yahoo.co.jp
Received: August 30, 2021; Accepted: September 13, 2021; Published: September 28, 2021
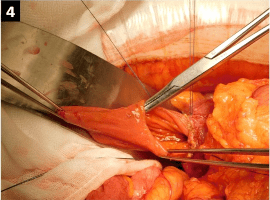
Citation: Shinoda T, Toshiyuki T, Nakashima T, et al. Recurrent Pancreatitis Due to an Intraluminal Duodenal Diverticulum. Clin Image Case Rep J. 2021; 3(8): 183.