")
")
Elior Moreh1,2*, Sheer Shabat1, Nurith Hiller2,3 and Efrat Suraqui1
1Physical Medicine and Rehabilitation Department, Hadassah Hebrew University Medical Center, Jerusalem, Israel
2Faculty of Medicine, Hebrew University, Jerusalem, Israel
3Radiology, Hadassah Hebrew University Medical Center, Jerusalem, Israel
*Corresponding author: Elior Moreh, Physical Medicine and Rehabilitation Department, Hadassah Hebrew University Medical Center, POB 24035, Jerusalem 92140, Israel. E-mail: elior@hadassah.org.il
Received: May 12, 2022; Accepted: May 20, 2022; Published: June 03, 2022
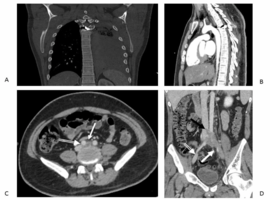
Citation: Moreh E, Shabat S, Hiller N, Suraqui E, et al. A Bullet in the Thoracic Spine and May-Thurner Syndrome. Clin Image Case Rep J. 2022; 4(5): 234.