")
")
L. Jay-Caillierez1*, B. Allaouchiche2 and F. Cotton3
1Lucille Jay-Caillierez, Hospices Civils de Lyon, Service d’Anesthésie Réanimation, Groupement Hospitalier Sud, F-69495, Pierre Bénite, France
2Bernard Allaouchiche, Hospices Civils de Lyon, Service d’Anesthésie Réanimation, Groupement Hospitalier Sud, F-69495, Pierre Bénite, France
3François Cotton, Hospices Civils de Lyon, Service de Radiologie, Groupement Hospitalier Sud, F-69495, Pierre Bénite, France
*Corresponding author: Lucille Jay-Caillierez, Hospices Civils de Lyon, Service d’Anesthésie Réanimation, Groupement Hospitalier Sud, F-69495, Pierre Bénite, France, Tel: +33478861476; E-mail: lucille.jay@chu-lyon.fr
Received: March 30, 2021; Accepted: April 07, 2021; Published: April 28, 2021
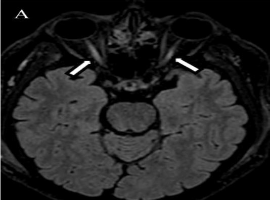
Citation: L. Jay-Caillierez, B. Allaouchiche, F. Cotton, et al. Acute Blindness After Lower Limb Injury. Clin Image Case Rep J. 2021; 3(3): 155.