A 72-year-old man presented with rapidly worsening ocular pain and vision loss within 24 hours after primary repair of a metallic open-globe injury. Examination revealed marked eyelid edema, conjunctival hyperemia, hypopyon, and elevated intraocular pressure. Initial ultrasonography was unremarkable, but repeat imaging demonstrated progressive vitreous opacities.
Despite prompt initiation of broad-spectrum antimicrobial therapy, guided by infectious disease consultation, the clinical course deteriorated with corneal melting, anterior chamber collapse, and dense vitritis, consistent with severe post-traumatic endophthalmitis.
Given the extensive involvement of both anterior and posterior segments, urgent combined surgical management was undertaken, including penetrating keratoplasty and pars plana vitrectomy.
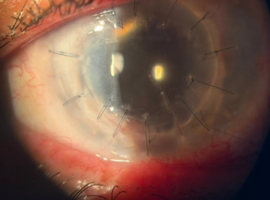
Figure 1 shows the preoperative anterior segment findings, characterized by corneal opacification, hypopyon, and structural collapse of the anterior chamber. Figure 2 demonstrates the postoperative appearance seven days after surgery, with restoration of anterior segment anatomy and resolution of intraocular inflammation.
This case highlights the fulminant nature of post-traumatic endophthalmitis and emphasizes the importance of early recognition and timely escalation to combined surgical intervention when anterior segment compromise precludes standard posterior segment management.
")
")