")
")
Tony Zhang1* and Peter Alan Barber2
1Neurology Registrar, Department of Neurology, Auckland City Hospital, 2 Park Road, Grafton, Auckland 1023, New Zealand
2Professor of Neurology, Department of Neurology, Auckland City Hospital, 2 Park Road, Grafton, Auckland 1023, New Zealand
*Corresponding author: Tony Zhang, Neurology Registrar, Department of Neurology, Auckland City Hospital, 2 Park Road, Grafton, Auckland 1023, New Zealand. E-mail: tonyz@adhb.govt.nz
Received: June 29, 2022; Accepted: July 07, 2022; Published: July 20, 2022
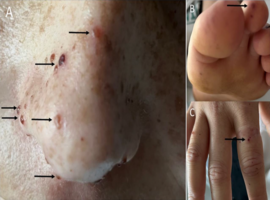
Citation: Zhang T, Barber PA. Diag(nose)ing Septic Emboli. Clin Image Case Rep J. 2022; 4(7): 247.