")
")
Abdullah Alabdulgader*
Congenital Cardiologist, Electrophysiologist, Saudi Arabia
*Corresponding author: Abdullah Alabdulgader, MD, DCH (Dublin), DCH (Edinburgh), MRCP (UK), ABP (CAMH), FRCP (Edinburgh), Pacing and Electrophysiology (University of Alberta-Canada). Senior Scientist, Congenital Cardiologist, interventional electrophysiologist and cardiac rhythm devices implanter, Psychophysiologist, Philosopher, World Gold Medal Awardee (Wosco-2012). Scientific Advisory Board Member (Heart Math Institute-USA).
E-mail: Alabdulgader.ep@gmail.com
Received: May 14, 2026; Accepted: June 01, 2026; Published: June 15, 2026
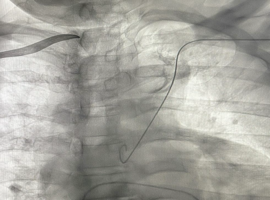
Citation: Alabdulgader A. Dynamic Fluoroscopic Recognition of Chronic Subclavian Vein Occlusion During CIED Implantation: Mechanobiological Remodeling and Functional Venous Patency. Clin Image Case Rep J. 2026; 8(3): 595.