A 61-year-old man with esophageal candidiasis treated with fluconazole presented with coffee-ground emesis and respiratory distress. On presentation, he was hypoxic, hypotensive, and tachycardic. Chest radiography demonstrated a left-sided hydropneumothorax.
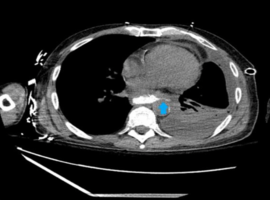
Non-contrast computed tomography (CT) of the chest demonstrated circumferential thickening of the thoracic esophagus with loss of surrounding fat planes, raising concern for severe esophagitis or underlying esophageal pathology. Pleural fluid analysis revealed an exudative effusion containing food particles and squamous cells, consistent with an esophago-pleural communication. Cultures grew Streptococcus salivarius. Subsequent CT confirmed a left-sided bronchoesophageal fistula (Figures 1 and 2). The patient was started on micafungin, and conservative medical management was pursued due to the distal location of the fistula. After two weeks, the patient made a full recovery.
While esophageal candidiasis is typically diagnosed endoscopically, this case highlights cross-sectional imaging findings that may suggest complicated esophageal infection and prompt early diagnostic consideration, particularly in critically ill patients.
")
")