")
")
Pretty Sara Idiculla*, Vinay Shet and Jobin Philipose
Mountain View Regional Medical Center, 4311 E Lohman Ave, Las Cruces, New Mexico
*Corresponding author: Pretty Sara Idiculla, MD, Mountain View Regional Medical Center, Las Cruces, New Mexico. E-mail: sarahidiculla.psi@gmail.com
Received: August 25, 2025; Accepted: September 08, 2025; Published: September 15, 2025
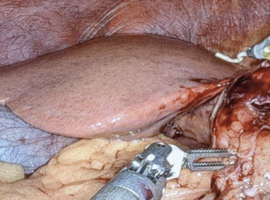
Citation: Idiculla PS, Shet V, Philipose J. Falciform Ligament Necrosis: A Rare Clinical Entity. Clin Image Case Rep J. 2025; 7(6): 575.