")
")
Calin Pop1* and Sabin Nemes Bota2
1Emergency Clinical County Hospital Baia Mare, “Vasile Goldis” University, Faculty of Medicine Arad, Romania
2Emergency Clinical County Hospital Baia Mare, Romania
*Corresponding author: Calin Pop, Emergency Clinical County Hospital of Baia Mare, George Cosbuc street nr 31, Baia Mare 430110, Romania, Tel: 0040744515794; E-mail: medicbm@yahoo.com
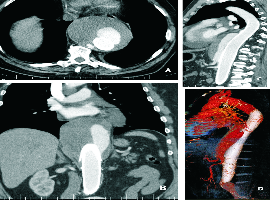
Citation: Calin Pop, Sabin Nemes Bota, et al. Giant Thoracoabdominal Aortic Aneurysm after EVAR. Clin Image Case Rep J. 2020; 2(2): 113.