A young child of 5.5 years of age presented with complaints of growth retardation. On examination, weight recorded was 11kg; height was 91 cm. Micropenis was noted with poorly formed scrotum and testicular volume of ~1cc each. On Clonidine stimulation test, GH values were found to be significantly low. LH, FSH and PRL values were also lower. Gross motor skills, language and social development was noted to be appropriate for age working diagnosis of GH deficiency was made and imaging was done.
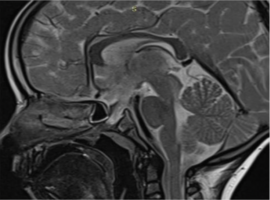
On CE-MRI sequences, posterior pituitary bright spot was not very well visualised with a bulbous soft tissue hypointense on T2 sequences protruding into the nasopharynx was noted. Floor of sella was absent with defect extending upto the nasopharynx. Defect size ~5.8mm. Rest of the brain parenchyma was found to be normal.
NCCT scan of the brain was done with bony window demonstrating the defect in the sphenoid bone spanning from sella to nasopharynx.
Persistent hypophyseal canal aka craniopharyngeal canal is a rare congenital skull defect. It has extension from the floor of the sella turcica to the nasopharynx. Etiology of this defect still remains unknown. We report the cross sectional imaging findings in a case of a young male child who presented with features of hypopituitarism.
Conventionally, it has been classified into 3 types.
TYPE I- incidentally detected thin persistent craniopharyngeal canal;
TYPE II- persistent craniopharyngeal canal with ectopic adenohypophysis;
TYPE IIIA- persistent CPC with cephalocele
IIIB- persistent CPC with Tumor
IIIC- Persistent CPC with both.
Possible complications related to this defect include CSF rhinorrhea, intracranial hypotension, meningitis, hypopituitarism and rarely can be associated with nasopharyngeal teratoma. Larger defects can also have other associated craniofacial anomalies like hypertelorism, cleft lip /palate, globe deformity, corpus callosum agenesis etc.
")
")