")
")
Rosita Sortino1*, Michael Schmid2, Luca Benigno1 and Walter Kolb1
1Department of Surgery, Kantonsspital St. Gallen, St. Gallen, Switzerland
2Department of Pathology, Kantonsspital St. Gallen, St. Gallen, Switzerland
*Corresponding author: Dr. Med. Rosita Sortino, Department of Surgery, Cantonal Hospital St. Gallen Rorschacherstrasse, St. Gallen, Switzerland, Tel: +41714949314; E-mail: rosita.sortino@kssg.ch
Received: November 26, 2020; Accepted: December 14, 2020; Published: January 03, 2021
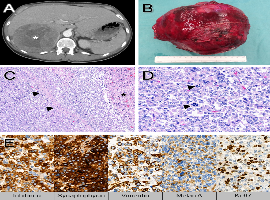
Citation: Rosita Sortino, Michael Schmid, Luca Benigno, et al. Primary Localized Giant Adrenal Cortical Carcinoma in a Young Adult Woman. Clin Image Case Rep J. 2021; 3(2): 134.