The patient is a 73-year-old male with a history of smoking, systemic steroid use, and high levels of stress related to employment who was referred to retina clinic due to detection of subretinal fluid in the right eye on optical coherence tomography (OCT) scan.
Visual acuity was 20/40 OD and 20/30 OS, intraocular pressure was 15 OD and 16 OS, and pupils were normal. Anterior slit lamp exam was unremarkable. Dilated fundus exam showed pigment mottling and epiretinal membrane (ERM) in the macula in both eyes.
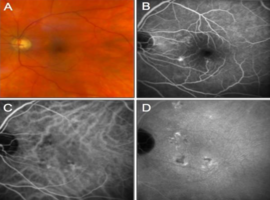
In the right eye, autofluorescence demonstrated perifoveal mottled hypo- and hyper-autofluorescence, OCT demonstrated ERM with subretinal fluid and thick choroid (407 ?m), intravenous fluorescein angiography (IVFA) demonstrated an expansile dot-pattern of leakage in the nasal and central macula, and indocyanine green angiography (ICGA) demonstrated persistent choroidal hypo-perfusion in the central macula (Figure 1). The fellow eye demonstrated similar findings (Figure 2). A diagnosis of central serous chorioretinopathy (CSCR) was made, and the patient underwent focal macular laser therapy to treat extrafoveal areas of leakage in the right eye. OCT of the macula three months later showed improving subretinal fluid (Figure 1).
This case was of interest due to the choroidal hypo-perfusion identified on ICGA, which may represent choroidal fibrosis in the setting of chronic CSCR. On OCT, the areas presumed to be fibrotic featured hypo transmission shadowing (Figure 1F, 1G). Choroidal fibrosis has not been widely described as a feature of this disease entity. To our knowledge, there has only been one recent case series published by Hansraj et al. describing similar findings in 4 patients with chronic CSCR [1]. We offer another case demonstrating that choroidal fibrosis may be a detectable feature in the chronic stages of this disease.
Keywords: Central serous chorioretinopathy; Choroid; CSCR; Fibrosis; Pachychoroid
")
")