")
")
Daniel Schöni1* and Alex Alfieri1,2
1Department of Neurosurgery, Cantonal Hospital of Winterthur, Winterthur, Switzerland
2Neurocenter of Southern Switzerland, Faculty of Biomedical Sciences, University of Southern Switzerland, Lugano, Switzerland
*Corresponding author: Daniel Schöni, Department of Neurosurgery, Cantonal Hospital of Winterthur, Winterthur, Switzerland. E-mail: daniel.schoeni@ksw.ch
Received: April 06, 2026; Accepted: April 20, 2026; Published: May 05, 2026
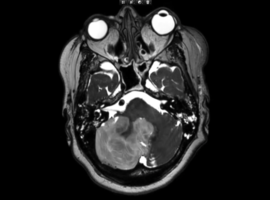
Citation: Schöni D, Alfieri A. Space-Occupying Cerebellar Infarction (SOCI): Intraoperative Visualization of Raised Intracranial Pressure and Cerebellar Tissue Prolapse. Clin Image Case Rep J. 2026; 8(2): 588.
The following video is related to this article (Video 1).