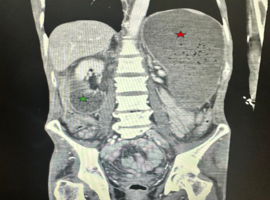
A 52-year-old mentally challenged, Native American male with past medical history of ESRD on HD, T2DM with neuropathy, essential hypertension, adrenal insufficiency, hypothyroidism, anemia of chronic disease, presented with diffuse abdominal pain, worse in the epigastrium, associated with nausea and vomiting, and a total weight loss of 118 lbs. CT of abdomen and pelvis showed severe fluid retention in the stomach and proximal duodenum, characteristic of SMA syndrome. Conservative management was initiated by nasogastric tube placement, which was pulled out by the patient and replacement was denied. The patient was started on TPN, with clinical improvement, and repeat CT showed resolution of previous findings. He was started on a clear liquid diet, slowly advanced to a mechanical soft diet as tolerated.
Patient discharge was planned; however, he developed two episodes of melena with a hemoglobin drop from 8 g/dL to 4 g/dL. After placing on a pantoprazole drip, he underwent emergent esophagogastroduodenoscopy (EGD) demonstrating a deep, actively bleeding esophageal ulcer treated with epinephrine injection and hemospray. After hemoglobin stabilization, he was started on a clear liquid diet which was advanced as tolerated.
SMA syndrome is rare with approximately 2400 reported cases by the year 2022. It is common among young adults, in particular females. Significant weight loss causes reduction of fat pad between the aorta and SMA, narrowing the aortomesenteric angle, resulting in duodenal compression. Diagnosis is confirmed with a CT scan by measuring the angles and endoscopy identifies complications. Malnutrition, dehydration, electrolyte abnormalities, gastric pneumatosis and portal venous gas, gastrointestinal hemorrhage, and gastric perforation are known complications. Recommended treatment is conservative with fluid resuscitation, electrolyte correction, TPN, NG tube insertion, small meals, and lateral decubitus position. If no improvement is noted, surgical management is recommended.
")
")