")
")
Ting-Wei Kao1, Yu-Feng Lin2, Chia-Lin Tseng2,3,4 and Nin-Chieh Hsu2,5*
1Department of Internal Medicine, National Taiwan University Hospital, Taipei 100, Taiwan
2Division of Hospital Medicine, Department of Internal Medicine, National Taiwan University Hospital, Taipei 100, Taiwan
3Department of Family Medicine, National Taiwan University Hospital, Taipei 100, Taiwan
4Institute of Health Policy and Management, College of Public Health, National Taiwan University, Taipei 100, Taiwan
5Department of Hospital Medicine, Taipei City Hospital Zhongxing Branch, Taipei 103, Taiwan
*Corresponding author: Nin-Chieh Hsu, National Taiwan University Hospital, Address: No.1, Changde Street, Zhongzheng District, Taipei 100, Taiwan. E-mail: chesthsu@gmail.com
Received: May 09, 2022; Accepted: May 17, 2022; Published: June 02, 2022
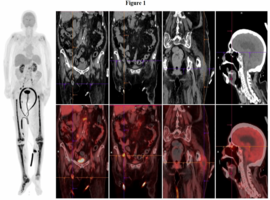
Citation: Wei Kao T, Feng Lin Y, Lin Tseng C, Chieh Hsu N, et al. Tibial Intravascular Large B-Cell Lymphoma. Clin Image Case Rep J. 2022; 4(5): 235.